Manoj Kumar K, Embryologist
Inside Embryo | Scientific and Medical Education
Introduction
Human embryology is the scientific study of development from fertilisation through the embryonic period, when the basic body plan and the primordia of most organ systems are established. It connects reproductive biology, cell biology, anatomy, genetics and physiology to explain how a single-celled zygote becomes a complex, organised human embryo.
Understanding human embryology is important for students, embryologists, clinicians, laboratory professionals, researchers and general readers. It provides the biological foundation for interpreting fertilisation, embryo culture, implantation, prenatal imaging, congenital anomalies and developmental research. It also clarifies why an embryo’s appearance at one moment cannot guarantee continued development, implantation, pregnancy or live birth.
This article follows development from fertilisation to the transition into the fetal period. It explains staging, germ-layer formation, neurulation, folding, organogenesis and extraembryonic support. It is an introductory educational overview rather than a clinical diagnostic guide, a laboratory standard operating procedure or a week-by-week prediction for an individual pregnancy. Related learning resources can be explored through the Inside Embryo Knowledge Hub.
Learning Objectives
- Define human embryology and distinguish post-fertilisation age from clinical gestational age.
- Identify the major preimplantation and postimplantation stages of early human development.
- Explain implantation, bilaminar-disc formation, gastrulation and neurulation.
- Describe the three primary germ layers and their broad developmental contributions.
- Explain how embryonic folding transforms a flat disc into a three-dimensional body form.
- Understand the purpose and limitations of Carnegie staging and embryo morphology.
- Relate basic embryology to IVF laboratory practice, prenatal medicine and congenital anomalies.
- Distinguish established embryology from emerging embryo-model and artificial-intelligence research.
Key Takeaways
- Human development is continuous, although named stages improve teaching and communication.
- Post-fertilisation age and gestational age use different starting points and should not be confused.
- Cleavage increases cell number without a comparable increase in the overall size of the conceptus.
- The blastocyst contains an embryoblast and trophectoderm with different developmental roles.
- Implantation is an active interaction between the blastocyst and a receptive endometrium.
- Gastrulation establishes ectoderm, mesoderm and endoderm and helps define the body axes.
- Neurulation, folding and organogenesis overlap rather than occurring as isolated events.
- Carnegie stages are assigned mainly by morphology, not by age or size alone.
- Embryo grading and developmental timing describe observations; they do not guarantee outcome.
- Human embryo research requires rigorous consent, oversight, transparency and compliance with local law.
Table of Contents
Definition and Overview
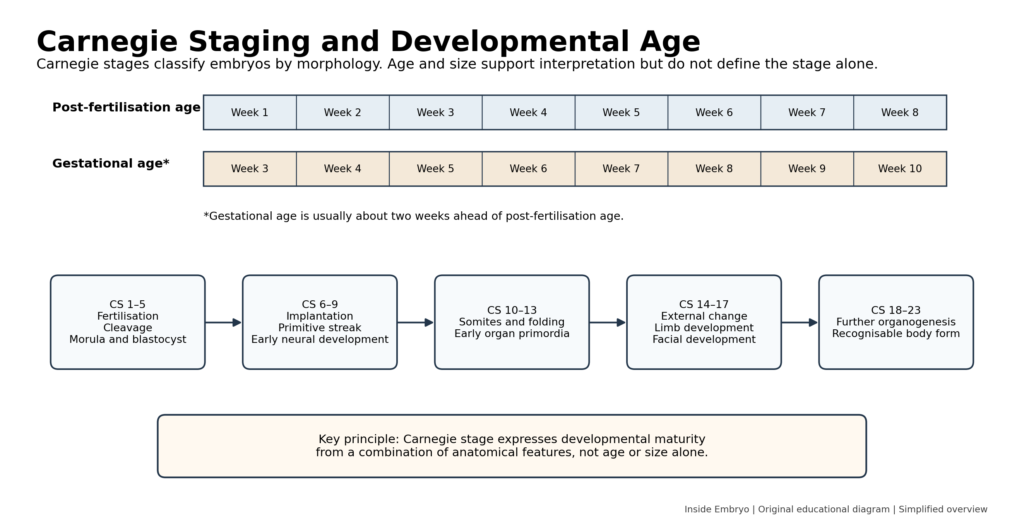
Human embryology examines the origin, transformation and spatial organisation of the conceptus during early prenatal development. The term conceptus includes the embryo or fetus together with associated extraembryonic structures. In standard anatomical usage, the embryonic period covers the first eight post-fertilisation weeks and is classified into 23 Carnegie stages. The fetal period begins after this interval and is dominated by growth, maturation and continued differentiation.[1,2]
Clinical pregnancy dating usually uses gestational age, counted from the first day of the last menstrual period. This convention generally places gestational age about two weeks ahead of post-fertilisation age, although the exact interval varies with ovulation and cycle characteristics. Clear writing should state which age convention is being used rather than using the word week without qualification.
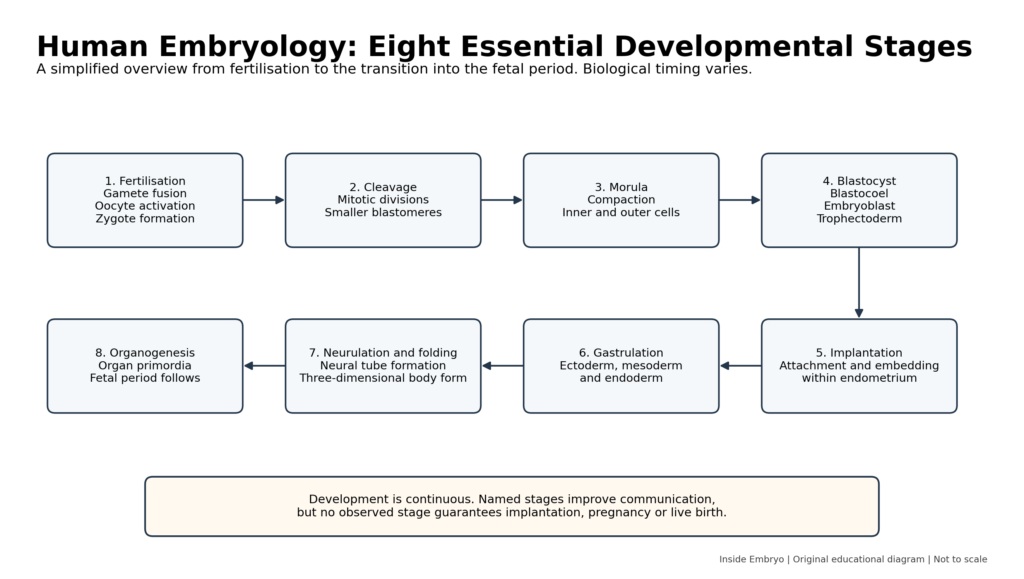
Embryogenesis is not a sequence of completely separate boxes. Cleavage, lineage specification, implantation, gastrulation, neurulation, folding, placental development and organogenesis overlap. A staged description is therefore a map of a continuous biological process, not a claim that all embryos reach a feature at an identical clock time.
Important Terminology
| Term | Clear meaning | Practical relevance |
| Conceptus | The embryo or fetus together with associated extraembryonic tissues. | Avoids using embryo when referring to the entire developing unit. |
| Zygote | The single cell formed after fertilisation and organisation of the parental chromosome sets. | The first cellular stage of a new developmental sequence. |
| Blastomere | A cell produced by cleavage of the zygote or early embryo. | Blastomere number and arrangement are observed in preimplantation development. |
| Morula | A compacted multicellular stage before a fluid-filled blastocoel is established. | Marks increased cell-cell interaction and inner-outer organisation. |
| Blastocyst | A preimplantation conceptus with a blastocoel, embryoblast and trophectoderm. | Capable of hatching and beginning implantation. |
| Embryoblast | The inner cell population of the blastocyst. | Contributes to the embryo proper and some extraembryonic structures. |
| Trophectoderm | The outer epithelial cell layer of the blastocyst. | Contributes substantially to trophoblast and placental tissues. |
| Implantation | Attachment and embedding of the blastocyst in the endometrium. | Establishes intimate embryo-maternal interaction. |
| Gastrulation | Cell movements that establish the three primary germ layers. | Creates the foundation of the body plan and organ systems. |
| Neurulation | Formation and closure of the neural tube from neural ectoderm. | Initiates central nervous-system organisation. |
| Organogenesis | Formation and early patterning of organ primordia. | A major feature of the embryonic period. |
| Carnegie stage | A morphology-based stage in the 23-stage human embryonic system. | Supports standardised description independent of age alone. |
Classification and Major Developmental Periods
| Period | Principal events | Scientific importance |
| Preimplantation development | Fertilisation, cleavage, morula and blastocyst formation | Cell division, compaction and first lineage organisation |
| Implantation and second week | Trophoblast differentiation, extraembryonic cavities and bilaminar disc | Embryo-endometrium interaction and early support systems |
| Gastrulation | Primitive streak and trilaminar-disc formation | Establishment of germ layers and body axes |
| Neurulation and folding | Neural plate/tube, somites and cranial-caudal/lateral folding | Transformation into a three-dimensional body form |
| Organogenesis | Development of organ primordia during weeks 3-8 after fertilisation | Foundation of most major organ systems |
| Fetal period | Growth and maturation after the embryonic period | Further differentiation, functional maturation and growth |
Scientific and Biological Background
Fertilization and zygote formation
Fertilisation is a regulated sequence involving sperm preparation, recognition of the oocyte coverings, membrane fusion and oocyte activation. The paternal and maternal genetic contributions are reorganised within the zygote. Fertilisation restores the diploid chromosome complement, establishes a new genomic combination and activates developmental processes. It should not be described as the sperm simply “entering an egg,” because multiple cellular and molecular events must be coordinated.
Cleavage, compaction and blastocyst formation
The zygote undergoes mitotic cleavage while enclosed by the zona pellucida. Cell number increases, but the overall conceptus remains approximately constrained, so individual blastomeres become progressively smaller. Compaction strengthens cell-cell contact and contributes to the distinction between inner and outer cell populations.
Fluid accumulation then creates the blastocoel. The resulting blastocyst contains the embryoblast, which contributes to the embryo proper, and trophectoderm, which contributes to trophoblast and placental development. Developmental timing varies, and cell number alone does not provide a complete measure of competence.[3]
Implantation and the bilaminar embryonic disc
After hatching from the zona pellucida, the blastocyst can interact with a receptive endometrium. Implantation involves apposition, adhesion and invasion. Trophectoderm differentiates into trophoblast populations, while endometrial stromal cells undergo decidualisation. Human implantation is interstitial and involves extensive tissue remodelling and signalling between embryonic and maternal compartments.[4]
During the second week, the embryoblast forms an epiblast and hypoblast, producing the bilaminar embryonic disc. The amniotic cavity, yolk-sac structures, extraembryonic mesoderm and chorionic cavity develop in parallel. These extraembryonic structures are essential to early support and organisation even though they do not all become part of the embryo’s body.
Gastrulation and establishment of the body plan
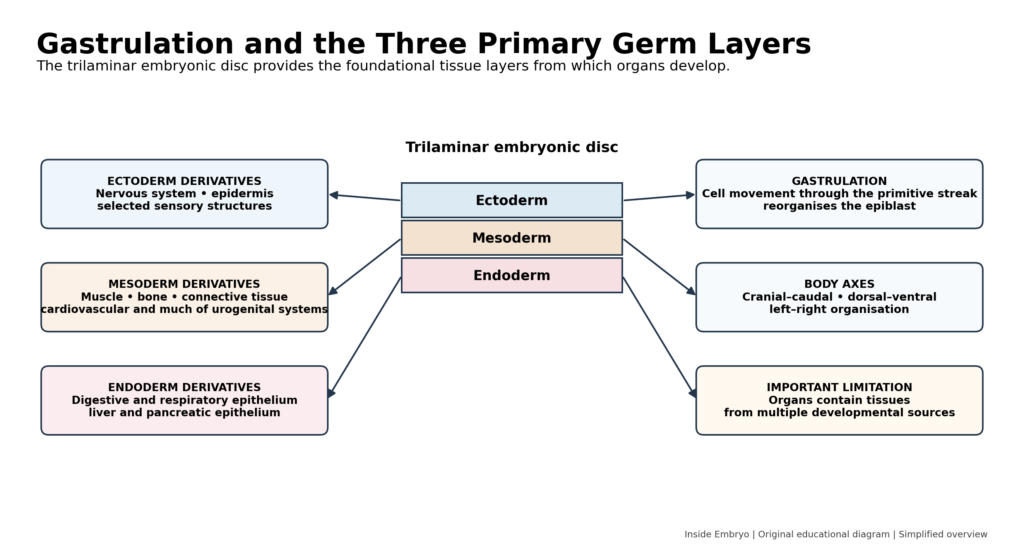
Gastrulation begins with formation of the primitive streak and coordinated movement of epiblast cells. Cells that displace the hypoblast form definitive endoderm; cells positioned between layers form intraembryonic mesoderm; and cells remaining in the epiblast become ectoderm. The process also contributes to cranial-caudal, dorsal-ventral and left-right organisation.[5]
The three germ layers are useful teaching categories, but organs are not built from one layer in isolation. An organ commonly contains epithelium, connective tissue, vessels, nerves and other components with different developmental origins.
Neurulation, somites and embryonic folding
Signals associated with the notochord and axial mesoderm induce overlying ectoderm to form the neural plate. Neural folds rise and fuse to create the neural tube, while neural crest cells emerge and migrate to many destinations. Neurulation begins during the third week and continues into the fourth.[6]
Paraxial mesoderm forms somites, which contribute to axial skeleton, skeletal muscle and dermis. At the same time, cranial-caudal and lateral folding transform the flat embryonic disc. Part of the yolk-sac endoderm becomes incorporated as the primitive gut tube, and the relationship between the heart, connecting stalk and developing body changes.
Organogenesis and the transition to the fetal period
Organogenesis extends across much of the embryonic period. Cardiovascular development begins early because diffusion alone becomes insufficient as the embryo grows. Limb buds, pharyngeal structures, sensory primordia, gut derivatives and urogenital structures undergo coordinated patterning. By the end of the eighth post-fertilisation week, the primordia of major organ systems are present, although they remain immature. The fetal period then emphasises growth and continuing differentiation.[7]
Placenta and extraembryonic development
Placental development begins during implantation and continues throughout pregnancy. Chorionic villi and maternal decidual tissues create a specialised exchange and endocrine interface. Maternal and embryonic or fetal blood normally remain in separate circulations, while gases, nutrients, waste products and signals cross the placental barrier through regulated processes. The placenta is an active organ rather than a passive filter.
Process, Mechanism and Developmental Workflow
1. Fertilisation: Competent gametes interact, fuse and activate zygote development.
2. Cleavage: Mitotic divisions create blastomeres while overall conceptus size remains constrained.
3. Compaction and morula formation: Cell adhesion and polarity establish inner and outer cellular environments.
4. Blastocyst formation and hatching: A blastocoel forms; embryoblast and trophectoderm become distinguishable.
5. Implantation and bilaminar-disc development: The conceptus embeds in endometrium while early embryonic and extraembryonic compartments organise.
6. Gastrulation: The primitive streak coordinates formation of ectoderm, mesoderm and endoderm.
7. Neurulation and folding: The neural tube, somites and three-dimensional body form develop.
8. Organogenesis and fetal transition: Organ primordia are established, followed by growth and maturation in the fetal period.
Clinical and Laboratory Significance
Embryology provides the framework for understanding prenatal imaging, congenital anomalies and the timing of developmental vulnerability. A structural difference may result from altered patterning, cell migration, proliferation, fusion, degeneration or tissue interaction. Identifying a mechanism requires more than knowing that an organ derives broadly from a particular germ layer.
In assisted reproductive technology, embryologists observe fertilisation, cleavage, compaction, blastocyst expansion and morphology. These observations support laboratory decisions but remain indirect. Morphology cannot reveal every chromosomal, genetic, epigenetic or metabolic property, and a normally developing laboratory-stage embryo does not guarantee implantation or live birth.
The updated ESHRE good-practice recommendations cover identification, traceability, embryo culture, fertilisation assessment, embryo transfer, cryopreservation, biopsy and emergency procedures. They combine available evidence with expert consensus and must be implemented within validated local quality systems.[8]
Embryology also supports responsible patient communication. Post-fertilisation age, gestational age, ultrasound dating and laboratory-developmental timing answer related but different questions. Apparent discrepancies may arise from dating assumptions, biological variation, measurement uncertainty or altered development and require professional assessment.
Factors Affecting Development or Interpretation
| Factor | Possible influence | Practical consideration |
| Chromosomal or genetic factors | May disrupt cell division, patterning, organogenesis or viability. | A detected variant requires context and, where appropriate, genetic counselling. |
| Maternal health and metabolism | Conditions such as poorly controlled metabolic disease may alter the developmental environment. | Risk depends on condition, timing, severity and management. |
| Medications and chemical exposures | Some agents can affect development during sensitive windows. | Do not stop prescribed medication without qualified medical advice. |
| Infections | Selected infections can interfere with embryonic or placental development. | Prevention, diagnosis and management are organism- and jurisdiction-specific. |
| Nutrition and micronutrients | Deficiency or excess may influence development. | Recommendations should follow current public-health and clinical guidance. |
| Oxygen, temperature and culture environment | Can affect metabolism and development in laboratory settings. | Use validated laboratory systems rather than universal internet parameters. |
| Embryo-endometrium interaction | Affects implantation and early placental development. | Neither embryo features nor endometrial tests alone prove implantation potential. |
| Biological and technical variation | Alters apparent timing, measurements and morphology. | Interpret repeated observations using appropriate reference standards. |
Interpretation of Findings
A developmental observation can indicate that a visible feature is present at the time of examination. It cannot prove that every preceding process was normal or that future development will continue. A blastocyst grade, ultrasound measurement or Carnegie-stage assignment summarises selected characteristics; it is not a complete biological diagnosis.
Chronological estimates should be separated from morphological staging. Carnegie stages use combinations of structural features. Embryos with a similar estimated age may differ in stage, and size alone is insufficient. The system contains 23 stages covering the first eight post-fertilisation weeks.[1,2]
Biological variation includes differences in fertilisation timing, cleavage patterns, implantation, growth and developmental pace. Technical variation includes culture conditions, observation intervals, imaging angle, fixation or specimen quality, ultrasound resolution and interobserver interpretation.
Professional assessment is required when findings are used to counsel about pregnancy viability, congenital anomalies, prenatal testing, embryo transfer or genetic risk. Educational descriptions should not be applied to personal scans, embryo photographs or laboratory records without appropriate clinical and laboratory context.
Common Errors and Misconceptions
| Error or misconception | Why it is incorrect | Correct understanding |
| An embryo is a miniature fully formed person. | Embryonic structures arise progressively through patterning, folding and organogenesis. | The early embryo is a dynamic developing system, not a small adult. |
| Pregnancy week and embryonic age are the same. | Clinical gestational age usually begins before fertilisation. | State whether age is gestational or post-fertilisation. |
| All embryos develop on an identical timetable. | Normal biological variation exists and observations are interval-dependent. | Use timing as a range and interpret morphology in context. |
| A high-grade embryo is genetically normal. | Morphology cannot directly establish chromosome or genetic status. | Grading describes visible features and has predictive limits. |
| Fertilisation guarantees implantation. | Continued development and embryo-endometrium interaction are also required. | Fertilisation is one step in a multistage process. |
| Each organ comes from only one germ layer. | Organs contain multiple tissue types with different origins. | Germ layers provide broad developmental contributions. |
| Carnegie stages are based mainly on embryo size. | Stages use combinations of morphological features. | Age and size support, but do not define, staging. |
| Embryo models are equivalent to natural embryos. | Models reproduce selected features and may lack complete organisation or potential. | Describe models by their demonstrated capabilities and limitations. |
Quality Control and Quality Assurance
Embryology laboratories require unambiguous patient and specimen identification, traceability and witnessing at critical steps. Labels and electronic records should connect gametes, embryos, devices, operators, dates, procedures and storage locations. Identification systems reduce risk but still require training, maintenance and incident review.
Incubators, microscopes, imaging systems, workstations, cryostorage equipment and environmental controls require qualification, monitoring and preventive maintenance. Media, consumables and reagents should be managed through approved suppliers, lot controls, storage requirements and documented acceptance procedures.
Staff need structured training, competency assessment and continuing professional development. Internal quality control, external quality assessment where available, audits, key performance indicators and corrective and preventive actions support consistent practice. No educational article can substitute for a validated laboratory standard operating procedure.[8]
Safety and Risk Management
Patient and specimen safety includes consent, privacy, correct identification, prevention of cross-contamination and secure data handling. Biological materials should be managed using appropriate infection-control and biosafety procedures. Chemical, ergonomic, electrical and equipment hazards also require documented controls.
Cryogenic storage introduces cold-injury, oxygen-displacement, pressure and storage-failure risks. Facilities require engineering controls, alarms, emergency plans, backup capacity and trained personnel. Specific cryopreservation conditions depend on validated protocols and manufacturer instructions and are not provided in this introductory article.
Embryo images and genetic results may contain sensitive information. Clinical material should not be shared through unsecured channels or reused for teaching, publication or artificial-intelligence development without suitable consent, de-identification and governance.
Evidence and Current Practice
Established human embryology includes cleavage, blastocyst formation, implantation, bilaminar- and trilaminar-disc development, neurulation, folding and organogenesis. Carnegie staging remains the standard morphology-based system for the embryonic period, although research continues to refine staging measurements and three-dimensional anatomy.[1,2]
Emerging research uses extended in-vitro culture, stem-cell-based embryo models, organoids, spatial transcriptomics, single-cell methods and advanced imaging to study stages that are difficult to observe directly. These systems can model selected processes but may not reproduce the organisation or developmental potential of an intact conceptus.
Artificial-intelligence tools are being investigated for embryo image analysis and developmental annotation. Consistency or predictive accuracy in a dataset does not prove clinical benefit, generalisability or freedom from bias. Such tools require transparent validation, appropriate oversight and continued professional judgement.
Advantages and Limitations of Embryology Methods
| Method | Advantage | Limitation |
| Classical morphology and Carnegie staging | Provides a common anatomical language across the embryonic period. | Depends on specimen quality and cannot reveal all molecular events. |
| Clinical ultrasound | Allows non-invasive assessment of pregnancy location, growth and selected anatomy. | Resolution and interpretation depend on timing, equipment and operator. |
| IVF embryo observation | Shows fertilisation and preimplantation morphology over defined intervals. | Laboratory appearance cannot guarantee genetic normality or live birth. |
| Genetic and molecular analysis | Can identify selected variants, chromosome findings or gene-expression patterns. | Sampling and assay limits remain; findings may not predict phenotype completely. |
| Embryo models and organoids | Permit controlled study of otherwise inaccessible processes. | Reproduce selected features and raise model-specific ethical questions. |
| Computational and AI analysis | Can organise complex imaging or molecular data. | Performance may change across populations, laboratories and devices. |
WHO Standards, Ethics and Legal Considerations
Human embryo research is ethically sensitive because it involves reproductive material, donor interests, potential future use and differing views about moral status. Consent should address the proposed research, storage, data use, genetic analysis, commercial involvement where relevant and whether recontact or withdrawal is possible.
The International Society for Stem Cell Research updated its Guidelines for Stem Cell Research and Clinical Translation in August 2025. The guidance calls for scientific rigour, specialised review, transparency and oversight of human embryo research and stem-cell-based embryo models, while explicitly stating that guidelines do not supersede local laws and regulations.[9]
National laws differ on embryo creation, storage, research duration, donation, genetic testing, embryo models and permissible clinical use. WHO guidance and professional recommendations may inform good practice but do not automatically replace legislation, licensing conditions, ethics-committee decisions or institutional policy.
Terminology should be accurate and respectful. The 2025 International Glossary on Infertility and Fertility Care provides updated consensus terminology intended to harmonise communication across science, care, policy and public education.[10]
Practical Summary for Different Readers
| Reader | Main learning focus | Responsible use |
| Students and beginners | Learn the sequence and the meaning of each stage before memorising organ derivatives. | Use recognised textbooks and anatomical atlases for deeper study. |
| Embryologists and laboratory professionals | Connect observed morphology with cell biology while respecting prediction limits. | Follow validated SOPs, competency requirements and current professional guidance. |
| Clinicians and healthcare workers | Use developmental timing to interpret prenatal findings and explain uncertainty. | Combine embryology with history, imaging, genetics and specialist assessment. |
| Patients and general readers | Understand that development involves many coordinated stages and natural variation. | Seek qualified advice for personal scans, tests, medications or pregnancy concerns. |
Frequently Asked Questions
When does the embryonic period begin and end?
In anatomical staging, development begins at fertilisation, and the embryonic period covers the first eight post-fertilisation weeks. Clinical gestational age uses a different starting point.
What is the difference between a zygote, morula and blastocyst?
A zygote is the initial single-cell stage. Cleavage produces blastomeres; compaction forms a morula; fluid accumulation and lineage organisation produce a blastocyst.
When does implantation occur?
Implantation begins after blastocyst hatching during early post-fertilisation development. Exact timing varies, and it is an ongoing interaction rather than a single instant.
Why are the three germ layers important?
Ectoderm, mesoderm and endoderm provide broad foundations for tissues and organs. Mature organs usually combine tissues from more than one developmental source.
What is a Carnegie stage?
It is one of 23 morphology-based stages used to describe human embryos during the first eight post-fertilisation weeks.
Does an embryo develop one organ at a time?
No. Nervous, cardiovascular, musculoskeletal, digestive and other systems develop through overlapping processes.
Can embryo grading confirm chromosome status?
No. Morphology and timing may be associated with outcome at a population level, but they cannot directly confirm chromosome status or guarantee live birth.
Are embryo models the same as embryos?
No. Stem-cell-based models reproduce selected developmental features and must be described according to their actual organisation and capabilities.
Why is human embryology difficult to study directly?
Many stages occur after implantation within maternal tissue, access is limited, and ethical and legal controls appropriately restrict research.
Can this article be used to interpret my ultrasound or embryo report?
No. Personal findings require interpretation by qualified professionals with access to the complete clinical and laboratory context.
Conclusion
Human embryology explains the continuous transformation from zygote to a structured embryo with established body axes and developing organ systems. Cleavage, blastocyst formation, implantation, gastrulation, neurulation, folding and organogenesis are interdependent processes supported by extraembryonic and placental development.
The field has direct relevance to reproductive laboratories, prenatal medicine, congenital-anomaly science and developmental research. Its observations also have limits: developmental age is estimated, morphology is incomplete, biological variation is expected and laboratory or imaging findings cannot guarantee outcome. Evidence-based interpretation therefore requires accurate terminology, appropriate staging, validated methods and qualified professional judgement.
A responsible introduction to human embryology should make development understandable without turning a continuous, variable biological process into a rigid timetable or presenting emerging models and technologies as established clinical tools.
References
1. O’Rahilly R, Müller F. Developmental stages in human embryos: revised and new measurements. Cells Tissues Organs. 2010;192(2):73-84. PMID: 20185898. Available from: https://pubmed.ncbi.nlm.nih.gov/20185898/
2. Flierman S, de Bakker BS, Oostra RJ. Discrepancies in embryonic staging: towards a gold standard. Life (Basel). 2023;13(5):1115. doi:10.3390/life13051115.
3. Khan YS, Ackerman KM. Embryology, Week 1. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; updated 2023 Apr 17. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554562/
4. Muter J, Lynch VJ, Brosens JJ. Human embryo implantation. Development. 2023;150(10):dev201507. doi:10.1242/dev.201507.
5. Muhr J, Ackerman KM. Embryology, Gastrulation. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; updated 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554394/
6. Rehman B, Muzio MR. Embryology, Week 2-3. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; updated 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK546679/
7. Donovan MF, Cascella M. Embryology, Weeks 6-8. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; updated 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK563181/
8. ESHRE Good Practice in the IVF Lab Working Group, Arroyo G, Barrie A, Coticchio G, et al. ESHRE recommendations on Good Practice in the IVF laboratory. Hum Reprod. 2026;deag096. doi:10.1093/humrep/deag096.
9. International Society for Stem Cell Research. Guidelines for Stem Cell Research and Clinical Translation. Version 1.2. Skokie (IL): ISSCR; 2025. Available from: https://www.isscr.org/guidelines
10. Zegers-Hochschild F, Dyer S, Racowsky C, et al. The International Glossary on Infertility and Fertility Care, 2025. Hum Reprod. 2026;41(6):892-921. doi:10.1093/humrep/deag029.
11. Singh R, Munakomi S. Embryology, Neural Tube. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; updated 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK542285/
12. Yamada S, Samtani RR, Lee ES, et al. Developmental atlas of the early first trimester human embryo. Dev Dyn. 2010;239(6):1585-1595. doi:10.1002/dvdy.22316.
Educational Disclaimer
Educational Disclaimer: This article is intended for scientific and educational purposes only. It does not replace professional medical advice, clinical judgement, institutional policies, validated laboratory protocols, manufacturer instructions, regulatory requirements or formal professional training. Laboratory and clinical procedures should be performed only by appropriately qualified personnel. Readers should consult current official guidance, applicable laws and qualified healthcare professionals when making clinical, laboratory or personal health decisions.