Introduction
Infertility is a reproductive health condition that affects people in every region of the world. The World Health Organization (WHO) estimates that approximately one in six people of reproductive age experience infertility during their lifetime [1–3]. Infertility may involve female reproductive factors, male reproductive factors, a combination of factors, or causes that remain unexplained after standard evaluation.
Understanding infertility requires more than studying hormones or reproductive organs. It also involves cellular biology, sperm function, oocyte quality, fertilization, embryo development, implantation, laboratory quality, ethics, and healthcare regulation. For patients, infertility can affect physical health, emotional well-being, relationships, finances, and future family-building decisions.
Modern fertility care therefore requires a coordinated approach involving clinicians, nurses, sonographers, andrologists, embryologists, laboratory scientists, counsellors, researchers, and regulatory authorities. Evaluation should be systematic and should consider all reproductive contributors rather than placing responsibility on one individual.
This article explains the biology of infertility, its major causes, the roles of semen analysis and embryology, the principles of assisted reproductive technology (ART), IVF laboratory quality, and the global ethical and regulatory issues surrounding fertility care.
Inside Embryo explains its approach to evidence selection and citation in the Scientific References and Sources Policy.
Learning Objectives
By the end of this article, readers should be able to:
- Define infertility and distinguish primary from secondary infertility.
- Explain the main biological stages required for human reproduction.
- Identify common female, male, combined, and unexplained infertility factors.
- Understand the roles of cellular biology, andrology, embryology, and the IVF laboratory.
- Describe the general workflow of an infertility evaluation.
- Recognize the importance of quality assurance, patient identification, consent, and traceability.
- Distinguish global professional guidance from national laws and institutional policies.
Key Takeaways
- Infertility is a condition of the male or female reproductive system and should not automatically be considered a “female problem.”
- A pregnancy requires coordinated oocyte development, sperm production, fertilization, embryo development, uterine receptivity, and implantation.
- Semen analysis is important, but one result alone does not provide a complete diagnosis of male fertility.
- Normal-looking gametes or embryos do not guarantee pregnancy, because morphology reveals only part of their biological competence.
- Not everyone with infertility requires in vitro fertilization (IVF); management depends on the identified cause, age, duration of infertility, medical history, and personal circumstances.
- IVF laboratory quality depends on validated procedures, trained personnel, stable environmental conditions, traceability, equipment monitoring, and risk management.
- WHO guidance and professional recommendations are not automatically legally binding. ART laws differ between jurisdictions.
- Infertility care should be evidence-based, respectful, confidential, non-discriminatory, and supported by valid informed consent.
Definition and Overview
WHO defines infertility as a disease of the male or female reproductive system characterized by failure to achieve pregnancy after 12 months or more of regular unprotected sexual intercourse [1,2]. Contemporary international terminology also recognizes that infertility may result from an impairment of a person’s reproductive capacity, including situations in which reproduction cannot occur without medical assistance [4].
Clinical evaluation may begin earlier when there are known risk factors, such as irregular or absent menstrual cycles, a history of pelvic disease, previous cancer treatment, reproductive surgery, sexual or ejaculatory dysfunction, severe semen abnormalities, or increasing reproductive age. Timing should be individualized rather than applied as a rigid rule [1,5,6].
Infertility is classified as:
- Primary infertility: No previous pregnancy has been achieved.
- Secondary infertility: At least one pregnancy has previously occurred, regardless of its outcome [2].
Infertility does not mean that pregnancy is impossible. It describes reduced or impaired reproductive capacity. The probability of pregnancy depends on the underlying cause, duration of infertility, reproductive age, general health, gamete quality, access to care, and the effectiveness and safety of any treatment used.
Important Terminology
| Term | Clear meaning | Practical relevance |
| Fertility | The capacity to establish a pregnancy | Describes reproductive potential rather than a guaranteed outcome |
| Infertility | Failure to achieve pregnancy after an appropriate period of exposure or because of impaired reproductive capacity | Indicates the need for clinical assessment when appropriate |
| Fecundability | The probability of achieving pregnancy during one menstrual cycle | Helps explain why conception may require several cycles even without disease |
| Ovulation | Release of a mature oocyte from an ovarian follicle | Necessary for natural fertilization in most menstrual cycles |
| Ovarian reserve | The remaining quantity of oocytes within the ovaries | Helps predict response to ovarian stimulation but does not directly measure natural fertility or oocyte quality |
| Spermatogenesis | Production and maturation of sperm cells within the testes | Disruption may reduce sperm number, movement, structure, or function |
| Azoospermia | Absence of spermatozoa in the ejaculate after appropriate laboratory examination | Requires further evaluation to distinguish obstruction from impaired sperm production |
| Fertilization | Fusion and activation of the oocyte and sperm genomes | Creates the zygote, the first cellular stage of a new embryo |
| Implantation | Attachment and invasion of the embryo into the receptive uterine lining | Essential for establishment of pregnancy |
| Assisted reproductive technology (ART) | Treatments involving laboratory handling of oocytes, sperm, or embryos to establish pregnancy | Includes IVF and related procedures |
| Unexplained infertility | Infertility in which standard evaluation has not identified a clear cause | Does not mean that no biological cause exists |
Classification and Major Causes
Infertility may arise at any point in the reproductive pathway. Multiple factors may be present simultaneously.
| Category | Examples | Possible reproductive effect |
| Ovulatory or endocrine factors | Polycystic ovary syndrome, hypothalamic dysfunction, thyroid or pituitary disorders, diminished ovarian function | Irregular follicular development, absent ovulation, or altered hormonal support |
| Tubal or pelvic factors | Tubal obstruction, pelvic infection, endometriosis, adhesions, previous surgery | Impaired sperm–oocyte transport, fertilization, or embryo transport |
| Uterine factors | Congenital abnormalities, selected fibroids, polyps, adhesions, endometrial disorders | May interfere with implantation or maintenance of pregnancy |
| Male reproductive factors | Reduced sperm concentration, poor motility, abnormal morphology, obstruction, hormonal dysfunction, testicular impairment | Reduced sperm delivery, movement, fertilizing capacity, or genetic integrity |
| Sexual or functional factors | Erectile, ejaculatory, coital, or pain-related difficulties | Reduced or absent exposure of sperm to the female reproductive tract |
| Combined factors | More than one male and female factor occurring together | Produces a cumulative reduction in reproductive probability |
| Unexplained infertility | Standard investigations appear acceptable | May reflect subtle gamete, fertilization, embryo, tubal, endometrial, or timing-related factors not detected by routine testing |
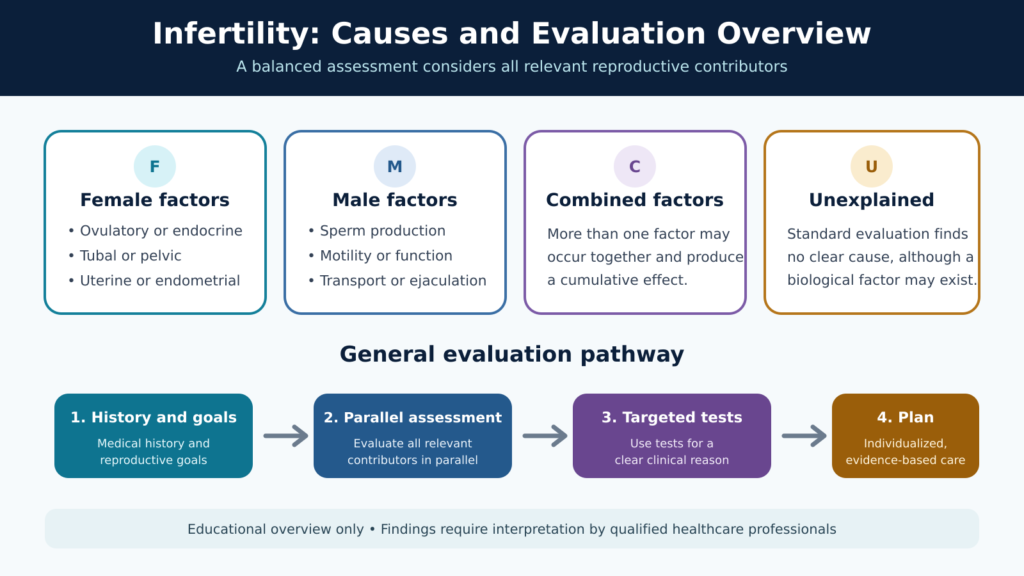
Figure 1. Infertility may involve female, male, combined, or unexplained factors; evaluation should consider all relevant contributors.
Female infertility may be associated with abnormalities of the ovaries, fallopian tubes, uterus, reproductive hormones, or pelvic environment. Male infertility may result from problems with sperm production, sperm transport, semen ejaculation, hormonal regulation, sexual function, or sperm quality [2,5,6].
Lifestyle and environmental exposures may influence reproductive health, but they should not be used to blame patients. Tobacco exposure, some infections, untreated sexually transmitted infections, certain medications, excessive heat exposure, occupational hazards, metabolic disease, undernutrition, obesity, and gonadotoxic treatments can affect fertility in selected individuals [1,2].
Scientific and Biological Background
Reproductive Biology
Human reproduction depends on coordinated activity of the hypothalamus, pituitary gland, ovaries, testes, reproductive ducts, uterus, and external reproductive organs.
In the female reproductive system, follicle-stimulating hormone supports ovarian follicle development. A dominant follicle produces increasing concentrations of oestrogen. A mid-cycle surge of luteinizing hormone contributes to final oocyte maturation and ovulation. After ovulation, the remaining follicular structure forms the corpus luteum, which produces progesterone to support the endometrium, or uterine lining.
In the male reproductive system, pituitary hormones act on the testes to support testosterone production and spermatogenesis. Sperm produced within the seminiferous tubules undergo further maturation as they pass through the epididymis. Seminal fluids from accessory glands combine with sperm during ejaculation.
Disturbance at any level of these hormonal systems can impair gamete production or reproductive function.
Cellular Biology
Oocytes and sperm are specialized reproductive cells called gametes. Unlike most human cells, which contain paired sets of chromosomes, mature gametes contain one set. This is achieved through meiosis, a specialized form of cell division.
Errors during meiosis may produce gametes with an abnormal chromosome number. The likelihood of some oocyte-related chromosome abnormalities increases with reproductive ageing. However, age is a probability-related factor and does not determine the outcome of an individual oocyte or embryo.
Mitochondria provide energy for cellular activities. They are important for oocyte maturation, early embryo development, and sperm movement. Cell membranes control movement of ions, nutrients, water, and signalling molecules. Disturbance of membrane stability can affect fertilization, embryo culture, and cryopreservation.
Reactive oxygen species are naturally produced during cellular metabolism and have some normal signalling functions. When their production exceeds antioxidant protection, oxidative stress may occur. Excessive oxidative stress can damage sperm membranes, proteins, mitochondria, and DNA. It may also affect oocytes and reproductive tissues. However, oxidative-stress tests and antioxidant treatments should not be used indiscriminately because methods, thresholds, and evidence vary.
Andrology and Sperm Function
Semen analysis is a core component of male fertility evaluation. The WHO laboratory manual provides standardized methods for assessing semen volume, sperm concentration, total sperm number, motility, morphology, vitality, and other characteristics [7].
Reference distributions in the WHO manual support standardized interpretation, but they are not absolute boundaries between fertility and infertility. A person with results below a reference value may still contribute to conception, while results within the reference range do not guarantee fertility.
Semen characteristics can vary between samples because of biological variation, illness, collection conditions, abstinence interval, incomplete collection, transport, temperature, laboratory technique, and time before analysis. Repeat testing may therefore be appropriate when an initial result is abnormal or inconsistent with the clinical situation [6,7].
Specialized assessments, including sperm DNA fragmentation or advanced sperm-function tests, may be useful in selected situations. They are not automatically required for every infertility evaluation, and their clinical value depends on the indication, method, quality controls, and whether the result will change management.
Embryology and Early Development
Following ovulation, sperm must reach the oocyte, undergo functional changes, interact with its surrounding layers, and participate in fertilization. The fertilized oocyte becomes a zygote.
The early developmental sequence includes:
- Oocyte maturation: The oocyte completes essential nuclear and cytoplasmic changes.
- Fertilization: Sperm and oocyte activation occur, followed by formation of the male and female pronuclei.
- Cleavage: The embryo divides into progressively smaller cells called blastomeres.
- Compaction and morula formation: Cells increase their contact and organize into a compact structure.
- Blastocyst formation: A fluid-filled cavity develops, with separation of the inner cell mass and trophectoderm.
- Hatching and implantation: The embryo emerges from the zona pellucida and interacts with the receptive endometrium.
Embryo morphology provides useful information about development, but it cannot directly reveal every chromosomal, metabolic, molecular, or implantation-related characteristic. The 2025 ESHRE/ALPHA Istanbul Consensus update provides standardized recommendations for evaluating oocytes, zygotes, and embryos while acknowledging important limitations [9].
General Infertility Evaluation Workflow
A safe and effective evaluation should be individualized, systematic, and as minimally invasive as reasonably possible.
- Clarify reproductive goals and history
- The clinician reviews duration of pregnancy attempts, previous pregnancies, menstrual history, sexual and reproductive history, contraception, medical conditions, surgeries, infections, family history, medications, occupational exposures, and previous fertility treatment.
- Evaluate all relevant contributors
- When sperm and oocytes are provided by different partners, both should usually be evaluated in parallel. Delaying male assessment can prolong diagnosis and treatment unnecessarily [5,6].
- Assess ovulation and endocrine function
- Menstrual patterns provide useful information. Hormonal or ultrasound assessment may be selected when cycles are irregular, ovulation is uncertain, or endocrine disease is suspected.
- Examine reproductive anatomy
- Ultrasound and other imaging methods may assess the ovaries, uterus, endometrium, and, when indicated, tubal patency. The choice of test depends on clinical history and local resources.
- Perform semen analysis
- Collection, transport, processing, examination, and reporting should follow standardized laboratory procedures. An abnormal result should be interpreted together with medical history and physical findings.
- Use targeted additional investigations
- Genetic, endocrine, infectious-disease, surgical, or advanced laboratory tests should be selected for a clear clinical reason. Routine use of poorly validated investigations may increase cost and anxiety without improving outcomes.
- Develop an individualized plan
- Findings are discussed with the patient or couple, including uncertainty, available management options, possible benefits, risks, costs, alternatives, and the consequences of delaying or declining treatment.
Management Approaches and Applications
Management depends on the cause of infertility and may include:
- Fertility awareness and appropriately timed intercourse.
- Treatment of identified endocrine or medical disorders.
- Ovulation induction for selected ovulatory conditions.
- Surgical treatment when a correctable anatomical abnormality is present and intervention is evidence-based.
- Intrauterine insemination in selected clinical situations.
- In vitro fertilization.
- Intracytoplasmic sperm injection (ICSI) when clinically indicated.
- Surgical sperm retrieval in selected cases.
- Donor sperm, donor oocytes, or donor embryos where legally permitted and personally acceptable.
- Fertility preservation before treatments that may impair reproductive function.
- Adoption or other family-building pathways.
- Supportive counselling or a decision not to pursue further treatment.
Not every additional test or laboratory “add-on” improves the probability of live birth. ESHRE recommends evaluating add-ons according to evidence of safety, effectiveness, and clinical relevance and ensuring that patients receive realistic information [11].
The Role of the IVF Laboratory
In IVF, oocytes are retrieved and handled in a controlled laboratory environment. Depending on the clinical indication, fertilization occurs through conventional insemination or ICSI. Embryos are cultured, assessed, selected for transfer or cryopreservation, and documented.
A competent IVF laboratory requires:
- Qualified and appropriately trained staff.
- Controlled access and defined workflow.
- Validated incubators, microscopes, warming systems, cryostorage equipment, and monitoring devices.
- Appropriate culture media, reagents, gases, consumables, and laboratory water.
- Monitoring of temperature, gas supply, incubator performance, and relevant environmental conditions.
- Patient and sample identification systems.
- Witnessing and traceability procedures.
- Validated cryopreservation and warming protocols.
- Emergency plans for power, equipment, gas, information-system, and cryostorage failures.
- Documentation, incident reporting, audits, and corrective and preventive actions.
The 2026 ESHRE Recommendations on Good Practice in the IVF Laboratory cover laboratory organization, staffing, safety, quality management, patient identification, traceability, sperm preparation, fertilization assessment, embryo culture, biopsy, cryopreservation, and emergency procedures [8]. These recommendations are professional guidance and must be adapted to national law, institutional policy, validated protocols, and manufacturer instructions.
Vitrification, Warming, and Cryostorage
Vitrification is a rapid cryopreservation approach designed to reduce damaging ice-crystal formation by combining cryoprotective solutions with very rapid cooling. Oocytes and embryos may be vitrified for fertility preservation, treatment planning, future embryo transfer, donor programmes, or other accepted clinical indications.
Successful cryopreservation depends on:
- Correct identification and labelling.
- Validated cryoprotectant exposure procedures.
- Precise control of time and temperature.
- Appropriate devices and storage systems.
- Secure transfer into cryogenic storage.
- Continuous inventory and tank monitoring.
- Validated warming procedures.
- Assessment of post-warming survival and developmental progression.
- Staff competency and emergency preparedness.
No single exposure time, cryoprotectant concentration, or carrier system should be presented as universally applicable. Laboratories must follow their validated procedure and the relevant manufacturer instructions [8,10].
Factors Affecting Reproductive and Laboratory Outcomes
| Factor | How it may affect outcomes | Practical consideration |
| Reproductive age | Influences oocyte quantity, chromosome-related risk, pregnancy probability, and miscarriage risk | Age should be discussed as a probability factor, not as an individual prediction |
| Ovarian and testicular function | Affects gamete production and hormonal support | Evaluation should identify treatable or medically important disorders |
| Sperm quality | May influence fertilization and embryo development | Interpret semen findings with clinical history and repeat testing when indicated |
| Oocyte and embryo competence | Influences fertilization, cleavage, blastocyst formation, and implantation | Morphology is informative but not a guarantee of genetic or developmental normality |
| Uterine and tubal factors | May affect gamete transport, embryo transport, or implantation | Select imaging and treatment according to evidence and symptoms |
| Laboratory environment | Temperature, pH, gas stability, air quality, and handling may affect cells | Monitor equipment and minimize unnecessary exposure outside controlled conditions |
| Operator competency | Technical consistency influences procedural reliability | Training, assessment, supervision, and continuing education are essential |
| Protocol adherence | Deviations may increase biological and identification risks | Use validated procedures and document deviations |
| Quality-management system | Supports consistency, traceability, and improvement | Review performance indicators, incidents, audits, and corrective actions |
Critical Control Points in Fertility Laboratories
| Critical control point | Why it matters | Possible risk | Preventive action |
| Patient and sample identification | Links biological material to the correct person | Sample or embryo mix-up | Use multiple identifiers, witnessing, and complete traceability |
| Semen collection and transport | Affects validity of analysis | Incomplete or altered sample | Provide clear instructions and document relevant collection details |
| Incubator stability | Supports embryo physiology | Temperature, gas, or pH disturbance | Continuous monitoring, alarms, maintenance, and backup plans |
| Media and consumables | Directly contact gametes and embryos | Toxicity, contamination, or performance variation | Approved suppliers, lot records, storage control, and validation |
| Cryostorage inventory | Preserves irreplaceable material | Mislocation, warming, or loss | Accurate mapping, audits, alarms, adequate tank management, and emergency procedures |
| Documentation | Provides clinical and legal traceability | Missing or incorrect records | Real-time recording, controlled forms, review, and secure data systems |
| Staff competency | Reduces technical variation and human error | Inconsistent or unsafe practice | Initial training, competency assessment, supervision, and reassessment |
Interpretation of Findings
Infertility results should not be interpreted in isolation. A menstrual hormone measurement, ultrasound finding, ovarian reserve marker, semen result, fertilization rate, or embryo grade represents only one part of a complex reproductive pathway.
Ovarian reserve tests mainly help estimate likely response to ovarian stimulation. They do not directly measure whether natural conception can occur and should not be used as population screening tests without a clinical indication [5].
Similarly, semen reference values describe population distributions rather than a strict fertile–infertile boundary [7]. Embryo grading helps laboratories describe development and prioritize embryos, but embryos with similar morphology can have different biological potential [9].
Unexpected findings should prompt review of pre-analytical, analytical, biological, and clinical factors before conclusions are made.
Common Errors and Misconceptions
| Problem or misconception | Why it is incorrect | Recommended response |
| “Infertility is usually the woman’s fault” | Male, female, combined, and unexplained factors can all contribute | Evaluate all relevant reproductive contributors without blame |
| “A normal semen analysis proves normal male fertility” | Routine semen analysis does not measure every sperm function | Interpret it with history, examination, and other findings |
| “Low ovarian reserve means pregnancy is impossible” | Reserve markers mainly estimate oocyte quantity and stimulation response | Provide individualized counselling based on the complete clinical picture |
| “IVF guarantees a baby” | Outcomes depend on many biological and clinical factors | Discuss probabilities, uncertainty, risks, and alternatives |
| “A high-grade embryo is genetically normal” | Morphology cannot directly confirm chromosome status | Explain the purpose and limitations of embryo grading |
| “Every available add-on improves success” | Many add-ons have limited, conflicting, or insufficient evidence | Discuss safety, evidence quality, cost, and whether the result changes care |
| “One abnormal laboratory result is a final diagnosis” | Biological and technical variation can affect results | Confirm collection quality and repeat or investigate when clinically justified |
Quality Control and Quality Assurance
Quality control consists of operational checks used to confirm that a process or instrument is performing as expected. Examples include temperature checks, calibration verification, control samples, reagent inspection, incubator monitoring, and cryostorage level monitoring.
Quality assurance is the broader system used to ensure that the entire service is safe, consistent, documented, and continually improving. It includes:
- Standard operating procedures.
- Staff training and competency assessment.
- Equipment qualification and preventive maintenance.
- Internal quality-control records.
- Participation in suitable external quality-assessment programmes.
- Supplier and reagent management.
- Performance-indicator monitoring.
- Witnessing and traceability.
- Internal audits.
- Incident and near-miss reporting.
- Root-cause analysis.
- Corrective and preventive actions.
- Management review and outcome evaluation.
Performance indicators should be interpreted in context. They are tools for identifying variation and improving processes, not instruments for blaming individual staff members or comparing laboratories without accounting for patient populations, clinical policies, and reporting methods [8].
Safety and Risk Management
Fertility services handle sensitive health information and irreplaceable biological material. Important risks include misidentification, infection exposure, chemical exposure, cryogenic injury, equipment failure, gas interruption, power loss, temperature excursions, data loss, unauthorized access, and inadequate consent.
Risk reduction requires layered controls rather than reliance on a single person or device. These controls include restricted access, personal protective equipment, alarm systems, backup power, emergency contacts, duplicate records, disaster-recovery plans, staff drills, secure electronic systems, and agreements with alternative facilities where appropriate.
Patients should be informed when a significant incident may affect their material, treatment, safety, or rights, according to applicable law and institutional policy.
Clinical and Laboratory Significance
Infertility evaluation can identify conditions that affect more than reproduction. Hormonal disorders, genetic conditions, infections, testicular disease, metabolic disorders, or uterine abnormalities may have wider health implications.
In ART, clinical decisions and laboratory performance are closely connected. Ovarian stimulation influences the number and maturity of oocytes available. Sperm quality may influence the choice of insemination method. Laboratory conditions affect gamete handling and embryo culture. Embryo-transfer strategy influences the risk of multiple pregnancy.
No single hormone level, semen parameter, embryo grade, incubator model, culture medium, or laboratory procedure independently determines live birth. Outcomes emerge from the interaction of patient biology, clinical management, laboratory practice, and chance.
Evidence and Current Practice
Well-established principles include simultaneous evaluation of relevant reproductive contributors, standardized semen analysis, investigation of ovulation and reproductive anatomy when indicated, and use of validated laboratory quality systems [1,5–8].
Common professional practice may vary because healthcare resources, patient characteristics, treatment costs, local expertise, and national regulation differ. Variation does not necessarily indicate poor practice, but departures from accepted guidance should have a clear scientific or clinical justification.
Evidence remains limited or conflicting for several advanced diagnostic tests and treatment add-ons. New technologies may improve observation, automation, or data analysis, but technical performance does not automatically prove improvement in cumulative live birth, patient safety, or cost-effectiveness.
Experimental approaches should be clearly identified as experimental and should be offered only with appropriate ethical review, consent, governance, and outcome monitoring.
Advantages and Limitations of Structured Infertility Care
| Advantages | Limitations |
| Can identify treatable reproductive or general health conditions | A clear cause cannot always be identified |
| Supports individualized management and informed decision-making | Tests cannot perfectly predict pregnancy or live birth |
| Provides access to fertility preservation and ART where appropriate | Cost and access differ greatly between countries |
| Standardized laboratory systems improve consistency and safety | Even high-quality laboratories cannot overcome every biological limitation |
| Counselling can reduce misinformation and unrealistic expectations | Treatment may involve physical, emotional, financial, and time burdens |
Global Standards, Ethics, and Legal Considerations
The WHO Guideline for the Prevention, Diagnosis and Treatment of Infertility, published on 28 November 2025, provides evidence-based global recommendations that countries may adopt or adapt when developing national fertility policies and clinical guidance [1]. WHO recommendations are not automatically legally binding.
Professional documents, such as the WHO semen manual and ESHRE laboratory recommendations, support good practice but do not replace national legislation, licensing conditions, accreditation requirements, professional scopes of practice, or institutional policies [7,8].
Laws differ substantially regarding:
- Eligibility and access to ART.
- Donor screening and donor anonymity.
- Payment or compensation for donation.
- Number of embryos transferred.
- Preimplantation genetic testing.
- Surrogacy.
- Legal parentage.
- Duration of gamete and embryo storage.
- Consent renewal and withdrawal.
- Posthumous use of reproductive material.
- Research use and disposal.
- Data protection and record retention.
- Cross-border transport of reproductive cells and tissues.
Valid informed consent should explain the proposed procedure, foreseeable risks, alternatives, limitations, storage arrangements, data use, financial responsibilities, and what may happen during separation, death, loss of contact, or withdrawal of consent, where relevant.
Confidentiality, non-discrimination, truthful outcome reporting, patient autonomy, child welfare, donor interests, and equitable access are important ethical considerations. Readers and professionals must consult the latest laws and official regulatory guidance applicable to their jurisdiction. This section does not constitute legal advice.
Practical Summary for Different Readers
| Reader group | What is most important to understand |
| Students and beginners | Infertility may involve multiple biological stages and either reproductive partner |
| Laboratory professionals | Identification, environmental control, validation, traceability, and documentation protect patients and samples |
| Clinicians and healthcare workers | Investigations should be targeted, coordinated, and interpreted within the complete clinical picture |
| Patients and general readers | Infertility is a medical condition, not a personal failure, and treatment outcomes cannot be guaranteed |
Frequently Asked Questions
1. When should a person seek an infertility evaluation?
Evaluation is commonly considered after 12 months of regular unprotected intercourse without pregnancy. Earlier assessment may be appropriate when there are irregular or absent periods, known reproductive disease, previous pelvic or testicular surgery, sexual dysfunction, previous gonadotoxic treatment, concerning semen findings, or age-related urgency. A qualified healthcare professional should determine the appropriate timing [1,5,6].
2. Does infertility always require IVF?
No. Some people may benefit from education about timing, treatment of an endocrine disorder, ovulation induction, surgery for a selected correctable condition, intrauterine insemination, or other management. IVF may be recommended when it provides a reasonable balance of effectiveness, safety, time, and cost for the specific clinical situation.
3. Can a person have infertility even after a previous pregnancy?
Yes. This is called secondary infertility. It may develop because of age-related reproductive changes, new medical conditions, infection, surgery, changes in semen quality, tubal or uterine disease, or factors that remain unexplained. A previous pregnancy does not guarantee that another pregnancy will occur [2].
4. Can semen quality change over time?
Yes. Semen characteristics can vary because of natural biological variation, fever, medication, illness, collection conditions, exposure history, and laboratory factors. One abnormal result may require confirmation. Persistent abnormalities should be evaluated by an appropriately qualified clinician or male reproductive specialist [6,7].
5. Does a good embryo grade guarantee implantation?
No. Embryo grading describes visible developmental features. Implantation also depends on chromosomal and molecular factors, embryo–endometrial interaction, uterine conditions, clinical management, and biological chance. Grading assists embryo prioritization but cannot guarantee implantation, pregnancy, or live birth [9].
6. What is unexplained infertility?
Unexplained infertility is diagnosed when standard evaluation has not identified a clear explanation. It does not mean that no biological problem exists. Current tests may not detect every disturbance in oocyte competence, sperm function, fertilization, embryo development, tubal transport, endometrial receptivity, or molecular communication.
7. Are sperm DNA fragmentation tests required for everyone?
No. These tests may provide additional information in selected cases, but methods and clinical interpretation vary. They should be ordered when there is a reasonable indication and when the result may influence counselling or management. Routine testing of every patient is not supported by all professional guidelines.
8. Are fertility supplements and antioxidants proven to improve outcomes?
Evidence differs between products, populations, doses, and outcomes. Some deficiencies require appropriate treatment, but routine use of multiple supplements does not guarantee improved sperm quality, oocyte quality, pregnancy, or live birth. Supplements can cause adverse effects or interact with medications. Patients should discuss them with a qualified healthcare professional.
9. How can patients judge whether a fertility laboratory is safe?
Patients may ask whether the centre is licensed where required, uses qualified staff, has documented identification and witnessing systems, monitors incubators and cryostorage, maintains emergency plans, reports outcomes responsibly, protects data, and provides clear consent information. Regulatory and accreditation arrangements vary by country.
Conclusion
Infertility is a complex reproductive health condition that may involve hormonal regulation, reproductive anatomy, gamete production, cellular function, fertilization, embryo development, implantation, or combinations of these factors. A responsible evaluation considers both male and female reproductive contributors, uses targeted investigations, and interprets results within the complete clinical context.
Andrology laboratories provide essential information about semen and sperm characteristics, while embryology laboratories support fertilization, embryo culture, cryopreservation, and other ART procedures. Their work must be supported by validated protocols, stable environmental conditions, competent staff, accurate identification, traceability, quality management, and emergency preparedness.
Tests, embryo grades, laboratory technologies, and treatments have important limitations. None can guarantee pregnancy or live birth. Evidence should be communicated honestly, particularly when tests or treatment add-ons have uncertain clinical value.
Globally, WHO guidance and professional recommendations provide important scientific frameworks, but legal requirements for ART, donation, genetic testing, storage, consent, data protection, and surrogacy differ between jurisdictions. Safe fertility care depends on evidence-based practice, valid consent, ethical responsibility, respectful patient communication, and continual quality improvement.
References
- World Health Organization. Guideline for the prevention, diagnosis and treatment of infertility. Geneva: WHO; 2025.
- World Health Organization. Infertility: Fact Sheet. Updated 28 November 2025.
- World Health Organization. Infertility Prevalence Estimates, 1990–2021. Geneva: WHO; 2023.
- Zegers-Hochschild F, Dyer S, Adamson GD, et al. The International Glossary on Infertility and Fertility Care, 2025. Fertility and Sterility. 2026;126(1):127–149. doi:10.1016/j.fertnstert.2026.02.022.
- Practice Committee of the American Society for Reproductive Medicine. Fertility evaluation of infertile women: a committee opinion. Fertility and Sterility. 2021;116(5):1255–1265. doi:10.1016/j.fertnstert.2021.08.038.
- American Urological Association; American Society for Reproductive Medicine. Diagnosis and Treatment of Infertility in Men: AUA/ASRM Guideline. Published 2020; amended 2024.
- World Health Organization. WHO Laboratory Manual for the Examination and Processing of Human Semen. 6th ed.. Geneva: WHO; 2021.
- ESHRE Good Practice in the IVF Lab Working Group. ESHRE recommendations on Good Practice in the IVF laboratory. Human Reproduction. 2026;deag096. doi:10.1093/humrep/deag096.
- Coticchio G, Ahlström A, Arroyo G, et al. The Istanbul Consensus update: a revised ESHRE/ALPHA consensus on oocyte and embryo static and dynamic morphological assessment. Human Reproduction. 2025;40(6):989–1035. doi:10.1093/humrep/deaf021.
- Practice Committee of the American Society for Reproductive Medicine. A review of best practices of rapid-cooling vitrification for oocytes and embryos: a committee opinion. Fertility and Sterility. 2021;115(2):305–310.
- ESHRE Add-ons Working Group. Good practice recommendations on add-ons in reproductive medicine. Human Reproduction. 2023. doi:10.1093/humrep/dead184.
Educational Disclaimer: This article is intended for scientific and educational purposes only. It does not replace professional medical advice, clinical judgment, institutional policies, validated laboratory protocols, manufacturer instructions, regulatory requirements, or formal professional training. Laboratory and clinical procedures should be performed only by appropriately qualified personnel. Laws, standards, and professional requirements may differ between countries and may change over time. Readers should consult the latest official guidance applicable to their jurisdiction. Individuals should consult an appropriately qualified healthcare professional for advice related to their specific medical history, fertility concerns, investigations, or treatment options.