Manoj Kumar K, Embryologist
Inside Embryo | Scientific and Medical Education
Introduction
Human reproductive biology is the study of the organs, cells, hormones and developmental events that make human reproduction possible. It connects anatomy with endocrine signalling, explains how oocytes and spermatozoa form, and follows the sequence from gamete transport and fertilisation to early embryo development and implantation. This foundation supports accurate understanding of fertility, reproductive-health evaluation and assisted reproductive technology.
Reproduction is not controlled by one hormone, organ, test result or embryo feature. It depends on coordination across reproductive systems, appropriate timing, competent gametes, a developing embryo and a receptive uterine environment. Even when individual findings appear normal, outcomes remain probabilistic rather than guaranteed.
This global introductory article does not diagnose infertility, predict an individual’s fertility or replace formal training. Readers can explore related foundations in the Inside Embryo Knowledge Hub.
Learning Objectives
- Define human reproductive biology and describe its major components.
- Identify the principal reproductive organs and their functional roles.
- Explain how the hypothalamic–pituitary–gonadal axis regulates ovarian and testicular activity.
- Compare oogenesis with spermatogenesis.
- Outline the biological sequence from ovulation and sperm transport to fertilisation and implantation.
- Recognise factors that may influence reproductive function and the limitations of isolated test results.
- Distinguish established reproductive biology from emerging or experimental research.
Key Takeaways
- Human reproduction requires coordinated endocrine, cellular, anatomical and developmental processes.
- Follicle-stimulating hormone and luteinising hormone regulate both ovaries and testes, but act through different target cells and functions.
- Oogenesis and spermatogenesis both involve meiosis, yet differ in timing, continuity and cellular output.
- Fertilisation is a multistep process involving competent gametes, recognition, membrane fusion and oocyte activation.
- Early embryo development proceeds through cleavage, compaction, morula and blastocyst formation before implantation.
- Implantation requires interaction between a developing blastocyst and a receptive endometrium.
- Fertility cannot be determined from one hormone value, one semen sample, one scan or one embryo observation.
- Clinical and laboratory findings must be interpreted in context by qualified professionals.
Table of Contents
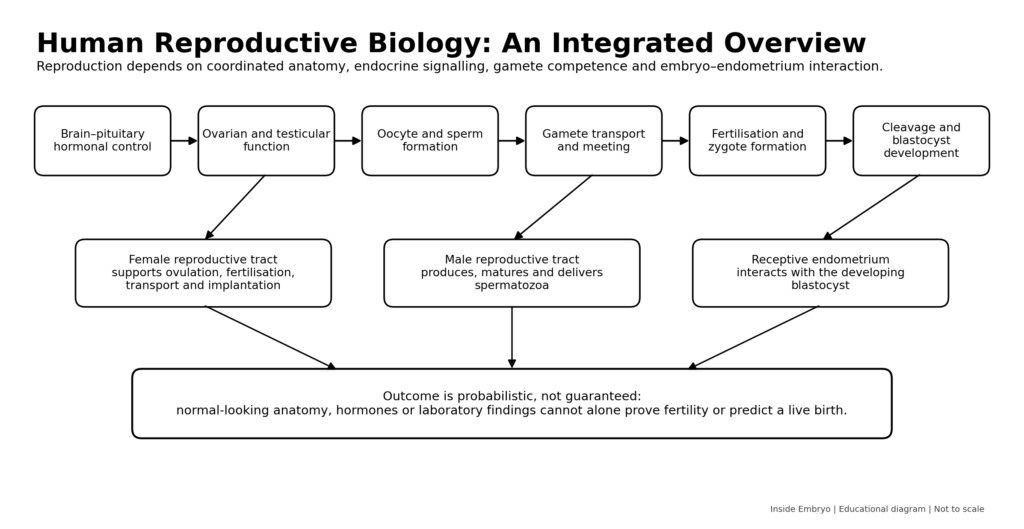
Figure 1. Integrated overview of the major systems and stages studied in human reproductive biology.
Definition and Overview
Human reproductive biology examines how the reproductive system develops, functions and contributes to a new individual. It includes gamete production, hormonal regulation, reproductive anatomy, fertilisation, preimplantation development, implantation and the biological establishment of pregnancy.
The World Health Organization places reproductive function within reproductive health, including physical, mental and social well-being related to the reproductive system. Reproductive biology therefore provides a basis for understanding puberty, menstrual function, fertility, contraception, pregnancy, infertility care and assisted reproductive technology.[1,2]
Fertility describes reproductive capacity, but biology does not reduce a person to a permanent binary label of “fertile” or “infertile.” Capacity varies over time and may be influenced by age, anatomy, endocrine function, health conditions, exposures and chance.
Important Terminology
| Term | Clear meaning | Practical relevance |
| Gamete | A haploid reproductive cell: an oocyte or spermatozoon. | Gametes contribute one set of chromosomes to the zygote. |
| Gametogenesis | The formation and maturation of reproductive cells. | Includes oogenesis in ovaries and spermatogenesis in testes. |
| Haploid | Containing one set of chromosomes. | Normal mature gametes are haploid. |
| Diploid | Containing two chromosome sets. | The zygote becomes diploid after gamete fusion. |
| Meiosis | A specialised cell division that reduces chromosome number and creates genetic variation. | Essential for forming haploid gametes. |
| Ovulation | Release of a secondary oocyte from an ovarian follicle. | Creates the opportunity for fertilisation in the reproductive tract. |
| Fertilisation | The ordered process through which sperm and oocyte unite and activate development. | Produces a zygote and initiates embryonic development. |
| Cleavage | Mitotic divisions of the early embryo without an overall increase in conceptus size. | Generates blastomeres and leads toward morula and blastocyst stages. |
| Blastocyst | A preimplantation embryo with an inner cell mass, fluid cavity and trophectoderm. | The stage that can hatch and begin implantation. |
| Implantation | Attachment and embedding of the blastocyst within the endometrium. | Establishes intimate embryo–maternal interaction. |
| Endometrium | The inner lining of the uterus. | Undergoes cyclic changes and supports implantation. |
| ART | Assisted reproductive technology. | Includes procedures in which oocytes or embryos are handled outside the body. |
Classification of the Field
Human reproductive biology can be organised into connected areas rather than isolated subjects.
| Area | Main components | Why it matters |
| Reproductive anatomy | Ovaries, uterine tubes, uterus, cervix and vagina; testes, epididymides, ducts, accessory glands and penis | Produces, transports and supports gametes and pregnancy. |
| Endocrine regulation | Hypothalamus, pituitary gland, gonads and feedback hormones | Coordinates puberty, cycles, steroid production and gametogenesis. |
| Cellular reproduction | Mitosis, meiosis, differentiation and cell signalling | Creates gametes and supports early development. |
| Preconception events | Follicular development, ovulation, sperm production and maturation | Prepare competent gametes and reproductive tissues. |
| Post-fertilisation events | Zygote formation, cleavage, blastocyst development and implantation | Initiate embryonic development and pregnancy. |
Scientific and Biological Background
Reproductive anatomy as a functional partnership
The ovaries produce oocytes and steroid hormones. The uterine tubes support gamete encounter and transport the developing conceptus toward the uterus. The uterus contains the endometrium, which changes under ovarian hormonal influence and supports implantation. The cervix and vagina contribute to sperm entry and transport.
The testes produce spermatozoa and androgens. Sertoli cells support developing germ cells in seminiferous tubules, while Leydig cells produce testosterone. Sperm mature further in the epididymis and travel through the ductal system; accessory-gland secretions form most seminal fluid.
Endocrine regulation
The hypothalamic–pituitary–gonadal axis provides central control. Pulsatile gonadotropin-releasing hormone (GnRH) stimulates pituitary release of follicle-stimulating hormone (FSH) and luteinising hormone (LH). Gonadal hormones and inhibins provide feedback.
In the ovary, FSH supports follicular growth, while LH contributes to steroid production, ovulation and corpus luteum function. Oestradiol and progesterone coordinate reproductive-tract changes. Cycle length varies, so ovulation should not be assumed to occur on an identical calendar day in every cycle.[3]
In the testis, LH stimulates Leydig-cell testosterone production, while FSH acts mainly through Sertoli cells. Spermatogenesis depends on coordinated endocrine and local cellular signalling, not testosterone alone.[4]
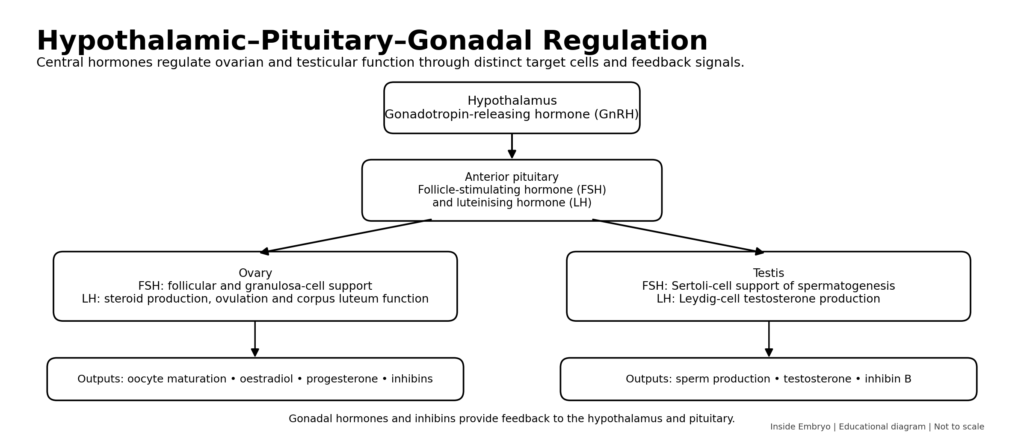
Figure 2. Simplified hypothalamic–pituitary–gonadal axis in ovarian and testicular physiology.
Gametogenesis
Oogenesis begins during fetal development. Primary oocytes enter meiosis and remain arrested within follicles. After puberty, selected follicles grow; the oocyte resumes meiosis around ovulation, and the released secondary oocyte completes the second meiotic division only if fertilisation proceeds.
Spermatogenesis begins functionally at puberty and includes spermatogonial renewal, meiosis and spermiogenesis—the remodelling of spermatids into specialised spermatozoa. Epididymal transit supports motility and fertilising function. Both processes require supportive somatic cells, appropriate hormones and tightly regulated gene expression.[4,5]
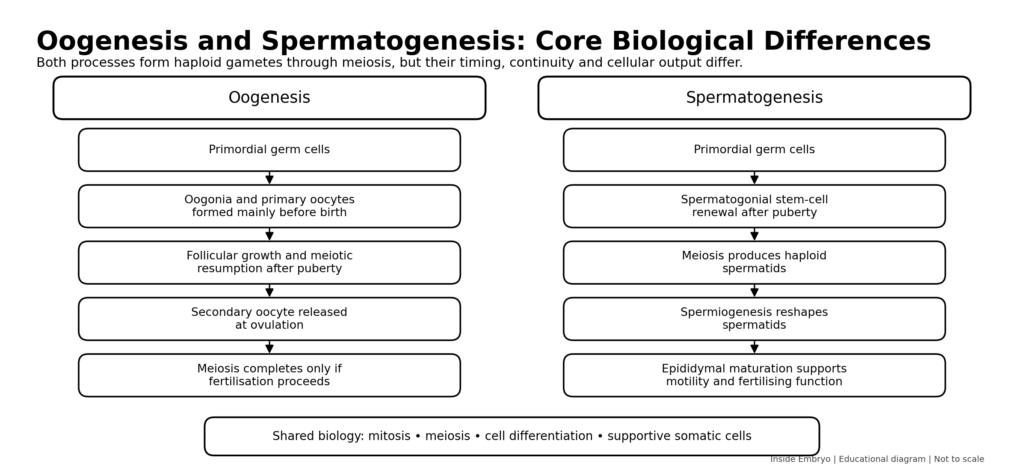
Figure 3. Comparison of the principal stages of oogenesis and spermatogenesis.
Fertilisation and early development
Before fertilisation, sperm undergo functional changes within the female reproductive tract known as capacitation. Fertilisation then involves ordered interactions with the oocyte coverings, membrane fusion and oocyte activation. Maternal and paternal chromosome sets are organised within the zygote; the event is a regulated cellular sequence rather than a simple collision.[6]
The zygote undergoes cleavage into blastomeres, followed by compaction, morula formation and blastocyst development. The blastocyst contains an inner cell mass and trophectoderm. These stages describe development but do not guarantee continued progression.
Implantation
Implantation requires interaction between a hatched blastocyst and an appropriately prepared endometrium. It is commonly described as apposition, adhesion and invasion. Endometrial stromal cells undergo decidualisation, a specialised transformation that supports and regulates implantation. Human implantation remains difficult to study directly.[7]
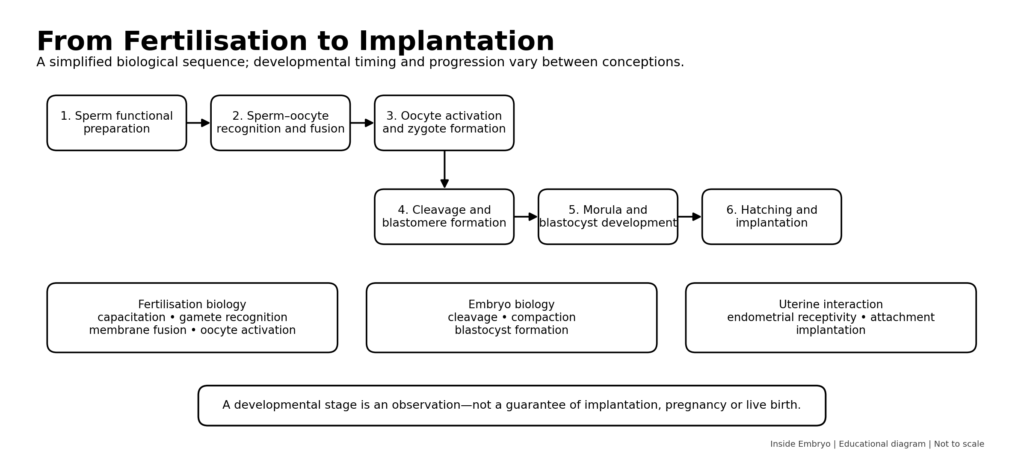
Figure 4. Educational workflow from sperm preparation and fertilisation to blastocyst implantation.
Process, Mechanism and Biological Workflow
1. Reproductive endocrine coordination: GnRH, FSH, LH, gonadal steroids and inhibins coordinate gamete production and reproductive-tract function.
2. Gamete development: Oocytes mature within ovarian follicles; spermatozoa develop in seminiferous tubules and mature further in the epididymis.
3. Ovulation and sperm deposition: An oocyte is released from the ovary, while sperm enter the female reproductive tract through intercourse or a medically assisted procedure.
4. Gamete transport: Tubal, uterine, cervical and sperm-related mechanisms influence whether competent gametes reach the same location.
5. Fertilisation: A sperm and oocyte interact, fuse and activate a new developmental programme, forming a zygote.
6. Preimplantation development: The conceptus undergoes cleavage, compaction, morula formation and blastocyst development.
7. Endometrial preparation: Ovarian hormones regulate endometrial growth and secretory transformation.
8. Implantation: The hatched blastocyst attaches to and embeds within the receptive endometrium, initiating deeper maternal–embryonic communication.
Clinical and Laboratory Significance
Reproductive biology helps clinicians organise evaluation logically. Ovulatory function, anatomy, semen characteristics, sexual function and health history are considered together rather than as isolated “female” or “male” problems. Guidance recommends parallel evaluation of relevant contributors when applicable.[8]
For embryologists and andrology professionals, this biology underpins specimen assessment, gamete handling, fertilisation observation and embryo culture. A semen analysis describes a sample; it does not independently prove fertility. Embryo morphology records appearance at a particular time and cannot guarantee implantation or live birth.
The same framework supports realistic counselling about biological variation, age-related change, treatment limits and the difference between population evidence and individual outcomes.
Factors Affecting Reproductive Processes or Outcomes
| Factor | Possible influence | Practical consideration |
| Age and reproductive stage | May influence ovarian reserve, oocyte competence, endocrine patterns and sperm characteristics. | Interpret in relation to the individual, not as an absolute prediction. |
| Anatomical conditions | May affect gamete production, transport, implantation or pregnancy maintenance. | Requires appropriate clinical assessment and imaging when indicated. |
| Endocrine disorders | Can disturb ovulation, steroid production or spermatogenesis. | Hormone results need timing, reference ranges and clinical context. |
| Genetic or chromosomal factors | May alter gamete development, fertilisation or embryo viability. | Testing is selective and should include qualified counselling. |
| General health and medications | Systemic illness or treatment may affect reproductive organs and hormones. | Medication changes require professional guidance. |
| Lifestyle and environmental exposures | Some exposures are associated with altered reproductive outcomes. | Association does not always prove direct causation. |
| Timing and frequency | Influence the chance that viable gametes meet. | Calendar prediction alone may be inaccurate. |
| Laboratory and technical variation | Collection, handling, equipment and observer variation can affect results. | Use validated methods, quality controls and repeat assessment when appropriate. |
| Biological chance | Not every gamete, fertilisation event or embryo progresses. | Normal findings do not guarantee conception or live birth. |
Interpretation of Findings
A reproductive observation usually answers a narrow question. Menstrual history may suggest regular cycles but cannot confirm every aspect of ovulation or oocyte competence. A hormone value reflects one signal at a defined time. A semen report characterises the tested sample, which may vary between collections.
Ultrasound, endocrine tests, semen analysis and embryo observations may identify patterns or reasons for further assessment. They cannot independently establish a complete diagnosis or guaranteed pregnancy probability. Reference intervals are not sharp borders between fertility and infertility because values may overlap.
Technical variation includes collection, transport, timing, assay method, equipment and observer interpretation. Biological variation includes cycle-to-cycle change, illness, incomplete samples, abstinence interval and age. Persistent reproductive symptoms, abnormal findings or difficulty conceiving require qualified assessment.
Common Errors and Misconceptions
| Error or misconception | Why it is incorrect | Correct understanding |
| Reproduction is mainly a female process. | Sperm production, transport and function are equally essential biological components. | Evaluate all relevant contributors without blame. |
| A regular menstrual cycle proves normal fertility. | Regular bleeding does not confirm tubal patency, oocyte competence, sperm function or implantation. | It provides one useful clue within a broader assessment. |
| One semen analysis gives a permanent fertility verdict. | Semen parameters vary and do not directly measure every aspect of sperm function. | Interpret a properly collected sample in clinical context; repeat when indicated. |
| Ovulation always occurs on day 14. | The follicular phase and total cycle length vary. | Estimate timing using the individual cycle and appropriate methods. |
| Fertilisation guarantees pregnancy. | An embryo must continue developing and implant successfully. | Fertilisation is one stage in a multistep process. |
| A high-grade embryo is a perfect embryo. | Morphology is an observation and cannot reveal every genetic or developmental property. | Use grading as one component of professional decision-making. |
| Stress alone causes most infertility. | Psychological stress may affect well-being and behaviour, but infertility has many biological causes. | Avoid blame and seek evidence-based evaluation. |
| Assisted reproduction bypasses all biology. | ART works through the same gametes, cell divisions and implantation biology. | Technology can assist steps but cannot guarantee outcomes. |
Quality Control and Quality Assurance
Although this is not a procedure article, quality principles matter whenever reproductive biology is measured clinically. Identification, traceability and witnessing reduce identification errors. Equipment monitoring, environmental control, reagent management and documented maintenance support reliable work.
Staff need training, competency assessment and continuing education. Laboratories should use validated methods, controlled documents, internal quality control, external quality assessment where available, audits and corrective and preventive actions. The WHO semen manual standardises semen examination, while ESHRE’s 2026 recommendations address quality, safety and traceability across IVF-laboratory activities.[9,10]
Educational explanations are not standard operating procedures. Laboratories must follow validated institutional protocols, current regulations and manufacturer instructions.
Safety and Risk Management
Reproductive care involves physical, psychological, biological, chemical, identification and data risks. Patient safety includes informed consent, respectful communication and prevention of avoidable harm. Staff safety requires infection control, safe handling, chemical controls, ergonomic practice and emergency preparedness.
Specimen safety depends on labelling, chain of custody, controlled storage, backup systems and incident management. Confidential reproductive and genetic information requires privacy controls. Cryogenic work adds cold-injury, oxygen-displacement and storage-failure risks that demand dedicated systems.
Evidence and Current Practice
Well-established biology includes the central roles of GnRH, FSH and LH; meiosis in gamete formation; sperm–oocyte fusion; cleavage; blastocyst development; and embryo–endometrium interaction during implantation. Professional recommendations translate parts of this knowledge into evaluation and laboratory standards.
Active research includes molecular predictors of gamete competence, non-invasive embryo assessment, endometrial tests, in-vitro gametogenesis, embryo models and artificial-intelligence systems. These approaches differ in maturity; some remain research tools, while others have uncertain clinical benefit. Emerging evidence must not be presented as established practice.
Practice also varies by jurisdiction, resources and patient circumstances. Scientific possibility does not automatically establish safety, effectiveness, ethical acceptability or legal permission.
Advantages and Limitations of an Introductory Biological Framework
| Strength | Educational value | Important limitation |
| Integrated framework | Connects anatomy, hormones, cells and development. | Cannot predict an individual outcome by itself. |
| Clinical relevance | Helps organise symptoms, tests and reproductive history. | Requires professional assessment and context. |
| Laboratory relevance | Explains why handling, timing and observation matter. | Educational biology is not a validated SOP. |
| Public understanding | Reduces myths, blame and oversimplification. | Introductory material cannot cover every disorder or treatment. |
| Research foundation | Supports understanding of new reproductive technologies. | Emerging findings may not translate into clinical benefit. |
WHO Standards, Ethics and Legal Considerations
WHO guidance places fertility care within sexual and reproductive health and rights. Ethical education should use inclusive language, protect privacy and avoid blame. People may pursue, postpone or decline reproduction for personal, medical, social or cultural reasons.
Assisted reproduction raises questions about consent, donation, embryo disposition, storage, genetic testing, access, parentage and research. Laws differ between countries and change over time. WHO and professional recommendations inform practice but do not replace national law, licensing requirements or institutional policy.
Gamete and embryo research requires applicable ethical review, consent and legal compliance. In-vitro gametogenesis and embryo models should be identified as experimental rather than established clinical options.
Practical Summary for Different Readers
| Reader | Main learning focus | Responsible use |
| Students and beginners | Learn the sequence: endocrine control → gametes → fertilisation → embryo development → implantation. | Use diagrams alongside standard textbooks and formal teaching. |
| Embryologists and laboratory professionals | Link observations to underlying cell biology and recognise interpretive limits. | Follow validated SOPs, quality systems and current professional guidance. |
| Clinicians and healthcare workers | Assess reproductive function as an integrated, shared process. | Combine history, examination and targeted testing; avoid isolated conclusions. |
| Patients and general readers | Understand that reproduction involves many coordinated steps and natural variation. | Seek qualified advice for personal symptoms, test results or treatment decisions. |
Frequently Asked Questions
What is the difference between reproductive biology and embryology?
Reproductive biology includes gamete production, hormones, reproductive anatomy, fertilisation and implantation. Embryology focuses more specifically on development after fertilisation, although the fields overlap.
Are fertility and reproductive health the same?
No. Fertility concerns reproductive capacity, while reproductive health includes wider physical, mental and social well-being related to reproductive functions and choices.
Does a normal menstrual cycle mean ovulation occurs every month?
Regular cycles make ovulation more likely, but they do not prove that every cycle is ovulatory or that all other reproductive factors are normal.
Can a normal semen analysis guarantee fertility?
No. It provides useful information about the analysed sample, but fertility also depends on sperm function, timing, the reproductive tract, the oocyte, fertilisation, embryo development and implantation.
Where does fertilisation usually occur?
It usually occurs within the uterine tube, but exact biological events and transport depend on functional gametes and reproductive-tract conditions.
When does an embryo become a blastocyst?
After cleavage and compaction, a fluid-filled cavity develops and cell populations begin to organise into inner cell mass and trophectoderm. Developmental timing varies.
Is implantation controlled only by the embryo?
No. Implantation requires coordinated interaction between the blastocyst and a hormonally prepared, biologically receptive endometrium.
Does reproductive age affect everyone in the same way?
No. Population trends are important, but individual reproductive biology and health history vary. Age should be considered with other clinical information.
Can one fertility test predict future pregnancy?
No single test can reliably predict natural conception or live birth for every person. Tests answer specific questions and require contextual interpretation.
Conclusion
Human reproductive biology provides an integrated explanation of how endocrine signals, reproductive organs, gametes and early developmental events work together. Oogenesis and spermatogenesis create specialised haploid cells; fertilisation combines their genetic contributions and activates development; cleavage produces the blastocyst; and implantation establishes a critical interaction with the endometrium.
This framework is clinically and scientifically important, but it has limits. Individual test values, semen parameters, scan findings and embryo observations describe only parts of a complex system. Evidence-based interpretation therefore requires biological context, validated methods and qualified professional judgement. A responsible introduction to human reproductive biology should support understanding without turning natural variability into certainty or educational information into personal medical advice.
References
1. World Health Organization. Reproductive health [Internet]. Geneva: WHO; [cited 2026 Jul 12]. Available from: https://www.who.int/southeastasia/health-topics/reproductive-health
2. World Health Organization. Sexual and reproductive health and rights [Internet]. Geneva: WHO; [cited 2026 Jul 12]. Available from: https://www.who.int/health-topics/sexual-and-reproductive-health-and-rights
3. Reed BG, Carr BR. The normal menstrual cycle and the control of ovulation. In: Feingold KR, Adler RA, Ahmed SF, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000–. Updated 2018 Aug 5. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279054/
4. O’Donnell L, Smith LB. Endocrinology of the testis and spermatogenesis. In: Feingold KR, Adler RA, Ahmed SF, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000–. Updated 2026 Jan 7. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279031/
5. Larose H, Shami AN, Abbott H, Manske G, Lei L, Hammoud SS. Gametogenesis: a journey from inception to conception. Curr Top Dev Biol. 2019;132:257-310. doi:10.1016/bs.ctdb.2018.12.006.
6. Siu KK, Serrao VH, Ziyyat A, Lee JE. The cell biology of fertilization: gamete attachment and fusion. J Cell Biol. 2021;220(10):e202102146. doi:10.1083/jcb.202102146.
7. Muter J, Lynch VJ, Brosens JJ. Human embryo implantation. Development. 2023;150(10):dev201507. doi:10.1242/dev.201507.
8. Practice Committee of the American Society for Reproductive Medicine. Fertility evaluation of infertile women: a committee opinion. Fertil Steril. 2021;116(5):1255-1265. doi:10.1016/j.fertnstert.2021.08.038.
9. World Health Organization. WHO laboratory manual for the examination and processing of human semen. 6th ed. Geneva: WHO; 2021. Available from: https://www.who.int/publications/i/item/9789240030787
10. ESHRE Good Practice in the IVF Lab Working Group, Arroyo G, Barrie A, Coticchio G, et al. ESHRE recommendations on good practice in the IVF laboratory. Hum Reprod. 2026;deag096. doi:10.1093/humrep/deag096.
11. Zegers-Hochschild F, Dyer S, Racowsky C, et al. The International Glossary on Infertility and Fertility Care, 2025. Hum Reprod. 2026;41(6):892-921. doi:10.1093/humrep/deag029.
About the Author
Manoj Kumar K is an embryologist, author and founder of Inside Embryo. His educational work focuses on human embryology, reproductive biology, gamete science, IVF laboratory learning, cryobiology, quality and safety, and responsible scientific communication. Inside Embryo is designed to make complex reproductive-science concepts clearer while maintaining appropriate professional and medical boundaries.
Learn more about the author’s scientific and educational background in the author profile of Manoj Kumar K.
Educational Disclaimer
Educational Disclaimer: This article is intended for scientific and educational purposes only. It does not replace professional medical advice, clinical judgement, institutional policies, validated laboratory protocols, manufacturer instructions, regulatory requirements or formal professional training. Laboratory and clinical procedures should be performed only by appropriately qualified personnel. Readers should consult current official guidance, applicable laws and qualified healthcare professionals when making clinical, laboratory or personal health decisions.
Nice information
Nice